"flu deaths" from 2014-2019 were confirmed to involve influenza virus. Dr. Biix announced this in March.
############################Hi Folks,
I thought this was a useful summary of COVID that JMU University Health Center provided, so I am sharing it.
G
>>>
Global cases now exceed 32 million. New global daily cases now average about 285,000. India continues to have the most new daily cases, averaging about 87,000.
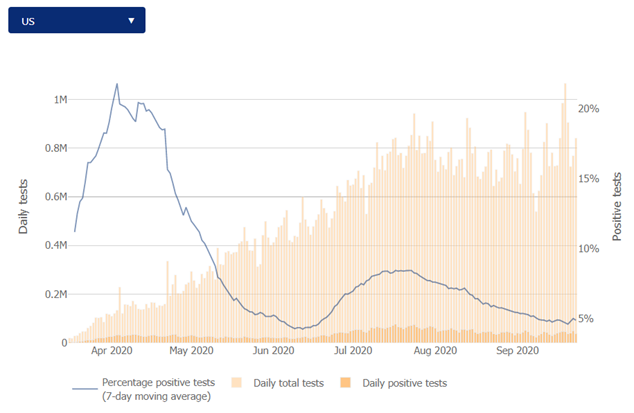
The US and Brazil continue in 2nd and 3rd place. Other South American countries (Argentina, Columbia) and some European countries are also seeing significant numbers. France and Spain are seeing a greater surge now than they did in the spring. On the positive side, the death rate has been significantly lower in these countries. The US 7-day moving average for test positivity rate has decreased to 4.9%, but daily testing still remains only around 800,000. Testing volume in the US continues to lag. However, these data reflect PCR testing. Antigen testing is becoming more available and being used more. States are just now adding these tests to their data.
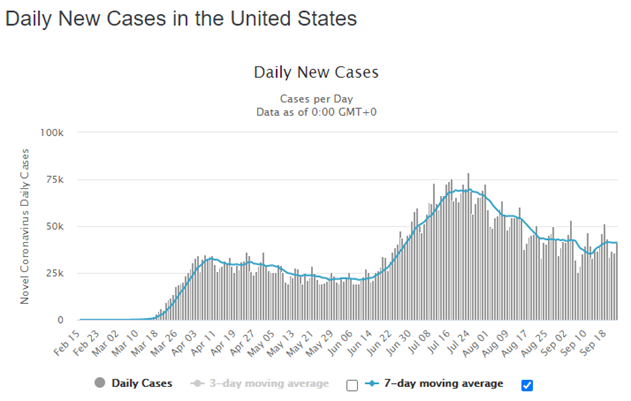
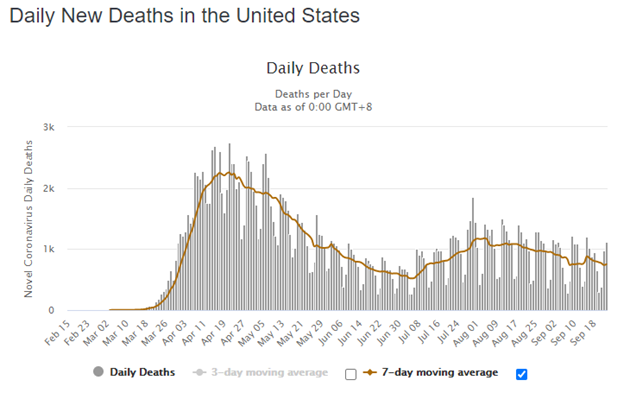
Nationally, total cases have now exceeded 7 million and are currently reported at 7,139,553. New daily cases continue to hover around 40,000. The average daily death rate is around 800. This is significantly lower than in April. Texas, California, and Florida remain as the top 3 states for new cases.
The Commonwealth reports a total of 143,492 cases and 3,113 deaths. The testing % positivity is currently at 5.3% which is a significant downward trend over the past 2 weeks.
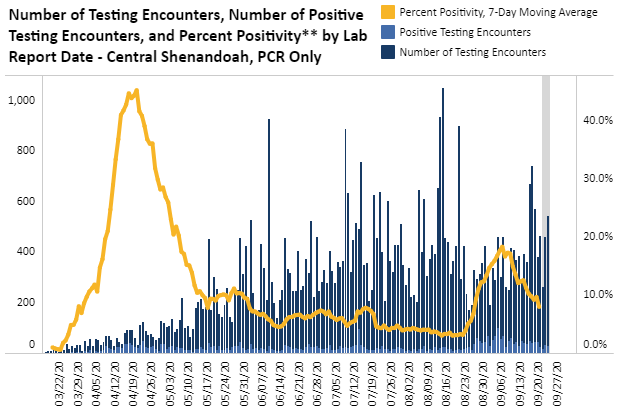
The Central Shenandoah Health District has also seen a significant decline in the 7-day moving average for test positivity, dropping from 18.3% on 9/6 to 7.9%.
Locality
Current total cases
New cases over the past 9 days
Prior 5 day data on new cases
Harrisonburg
2564
518
233
Rockingham County
1403
199
90
Augusta County
472
38
28
Staunton
250
31
30
Waynesboro
257
9
14
Shenandoah County
804
13
9
Page County
389
13
10
At JMU we are seeing fewer positive test and fewer people reporting a positive test performed elsewhere. However, we are also seeing fewer people get tested and therefore our 7-day average test positivity remains around 17%. All cases occurring in employees have been a result of either non-JMU related exposure or employee to employee (rather than student to employee) exposure. The reports are that face mask use in the academic settings has been very good. This significantly accounts for a lack of transmission between student and faculty.
Vaccine development continues with new vaccines being developed and entering clinical trials. Two of the vaccines that are furthest along in development are m-RNA vaccines (Moderna and Pfizer). However, there is a very interesting and concerning logistic related to these vaccines-the cold chain storage required. These vaccines require storage at -94 degrees Fahrenheit (yes, minus 94). Transport would require storage in dry ice. These vaccines last 24 hours at refrigerated temperatures between 36.6-46.4 Fahrenheit. In contrast, vaccines under development by Sanofi and Novavax are stable for months at typical refrigerated temperatures.
Johnson & Johnson has a single dose vaccine entering phase 3 trials while Merck and Sanofi (both well-known and well-respected in vaccine development) have vaccines in development and entering clinical trials. An important factor is the corporate knowledge, infrastructure, and ability of these two companies to both vaccine development and large-scale production. They may be late in the game but they should not be counted out. This article covers some information about vaccines in trials and development.
It seems very unlikely there will be a single winning vaccine-at least in the beginning. Time will tell which vaccine approach seems to work best with the optimal immune response and duration.
As an aside, recently the head of the CDC (Robert Redfield) commented that mask wearing was likely to be more effective than any vaccine. “I might even go so far as to say that this face mask is more guaranteed to protect me against COVID than when I take a COVID vaccine,” Redfield said while testifying before the Senate Subcommittee on Labor, Health and Human Services on expectations around the release of COVID-19 vaccines. He was not indicating that vaccine are not likely to be effective but instead on the value of masks as a preventative measure. He may also have been forecasting the need for mask use even when vaccines are available.
Enjoy the beautiful weekend!
Andy Guertler
Andrew T. Guertler, MD
Medical Director
University Health Center
James Madison University
To unsubscribe from the TOK-SOCIETY-L list: write to: mailto:[log in to unmask] or click the following link: http://listserv.jmu.edu/cgi-bin/wa?SUBED1=TOK-SOCIETY-L&A=1


james lyons-weiler, phd